Olecranon Stress Fracture
STRESS FRACTURE PATHOLOGY:

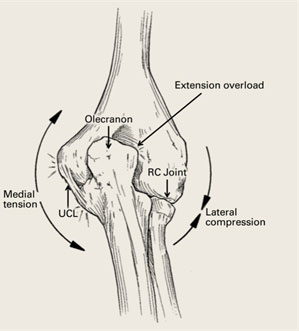
- As the elbow is forced into extension at the end of throwing cycle, there is a shearing force across the back of the elbow at the olecranon. This repetitive loading leads to compression in the posterior elbow.
- In the adolescent overhead athlete these forces lead to separation of the olecranon ossification center and if left untreated this can develop into an unfused olecranon apophysis and ultimately a symptomatic nonunion
- In the skeletally mature (adult) this can result in formation of bone spurs (osteophytes) and pain along the posterior medial aspect of the elbow known as valgus extension overload.
- In both adolescents and adults, this repetitive trauma can result in stress reactions or even stress fractures into the olecranon

DIAGNOSIS OF OLECRANON STRESS FRACTURE:
- Throwers will typically describe pain at follow-through and may have difficulty with accuracy and velocity
- Physical exam frequently demonstrates inability to fully extend (straighten) the arm. There may also be point tenderness over the olecranon exacerbated by percussion or vibration
- The “Bounce Test” or forced extension of the elbow can reproduce posterior pain
- Radiographs may demonstrate linear sclerosis, fracture lines, or periosteal bone formation. Contralateral films can help determine amount of closure
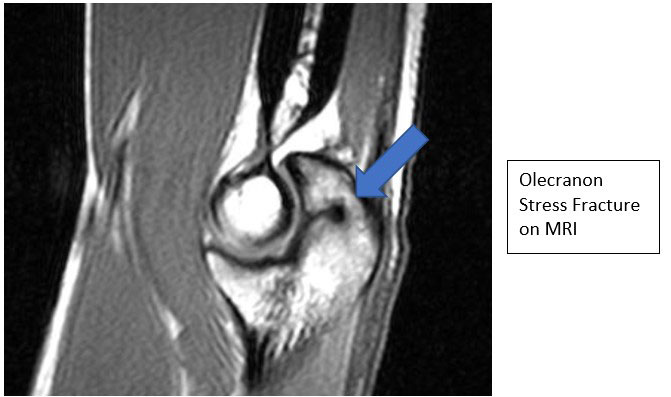
- MRI, CT and Bone scan can help establish diagnosis if x-rays are normal
TREATMENT:
- Treatment is based on patient’s skeletally maturity and fracture pattern
- Nonoperative management may be recommended when stress injuries/reactions are present without visible fracture lines. This typically consists of a period with cessation from throwing and activity modification until the fracture heals
- Younger athletes with less than 50% contralateral physeal closure may also respond to nonoperative treatment
- Older athletes are frequently treated with surgery if there is marked sclerosis adjacent to the physeal line, greater than 5mm apophyseal widening or other physis is closed
- Conservative care is rarely successful once visible on plain radiographs
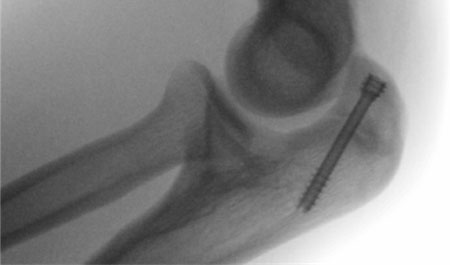
- Surgical treatment typically consists of partially threaded compression screws placed perpendicular to the facture line along the longitudinal axis of the ulna
POST OP:
- ROM initiated within 1-2 weeks with progression to full ROM as tolerated
- Non-weight bearing precautions and limiting resisted elbow extension until fracture is healed
- Interval throwing can begin once fracture is healed (typically between 8-12 weeks) and return to sport at 3-6 months