Medial Epicondyle Avulsion Fractures/Apophysitis

- The medial elbow is subject to significant force throughout the throwing cycle, specifically in the late cocking and early acceleration phases. The medial epicondyle is the “knob” on the inside part of our elbow and is the attachment site for many important ligaments and muscles.
- Skeletal immaturity makes adolescent players prone and vulnerable to throwing injury and overuse. In fact, nearly one-third of youth baseball pitchers will experience shoulder or elbow pain during the season. This is multifactorial, but the imbalance in strength between open physis (“growth plate”) and the attached tendons and ligaments coupled with repetitive strenuous force imparted by overhead throwing put adolescent throwers at particular risk for physeal injuries.
- In the growing athlete the ligamentous structures are actually 2-5x stronger than the open physes (growth plates). This means that both static (UCL) and dynamic (flexor-pronator mass) stabilizers inserting on the medial epicondyle, impart all forces to the medial epicondylar physis (growth plate)
- The term “Little Leaguer’s Elbow” can encompass a number of pathologic conditions in the skeletally immature including medial epicondylar apophysitis, physeal widening, fractures, posteromedial impingement, capitellar osteochondritis dissecans, stress lesions of the proximal ulna, nonunion or stress fractures of the olecranon, or abnormal persistence /widening of the ulnar physis into skeletal maturity
- Overuse remains the common thread throughout adolescent elbow injuries which provides an important opportunity for prevention to play a role in treatment strategy
- Good pitching mechanics have been proven to generate lower shoulder and elbow torques, lower joint loads and greater efficiency
- Two distinct conditions can affect the medial aspect of the skeletal immature elbow in the throwing athlete.
Medial Epicondyle Apophysitis
- Medial epicondyle appophysitis refers to a chronic inflammatory state where the muscles and tendons attach to the inside of the elbow
- This is an overuse injury as a result of repetitive strain across the medial elbow and associated with improper mechanics
- This typically presents with progressive medial elbow pain in overhead athletes 10 years or younger
- Pain in the late cocking and early acceleration phase is common as this is the highest valgus loads on the elbow
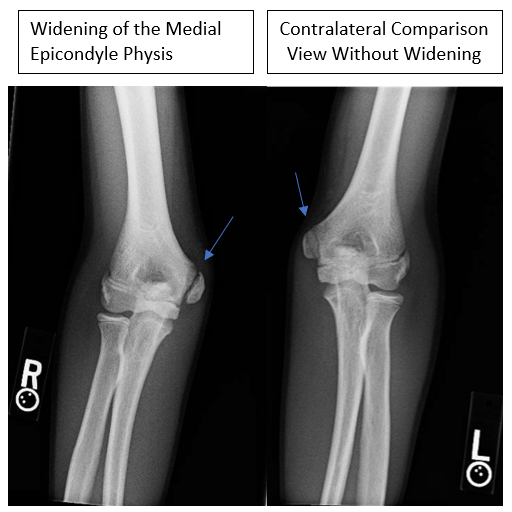
- X-rays typically demonstrate widened physis and sclerosis of the apophysis. Comparison films of the contralateral extremity can be very helpful for subtle differences
- Treatment is nonoperative with abstinence from throwing and a period of rest for 6-12 weeks. Throwing can begin once strength is symmetric and patient is completely symptom free

Medial Epicondyle Avulsion Fractures
- True fractures about the medial epicondyle typically occur between the age of 10-14 years
- This is a result of an acute injury typically associated with a discrete event such as a fall or a single throw
- This is not an overuse injury, but instead a result of the older athlete generating enough force to overwhelm the closing physis
- Pre-existing pain or chronic overuse history is NOT usually present
- Swelling is much more pronounced than with apophysitis and may have a loss of motion
- Patient is typically unable to continue to throw and tingling into the pinky and ring fingers may be present
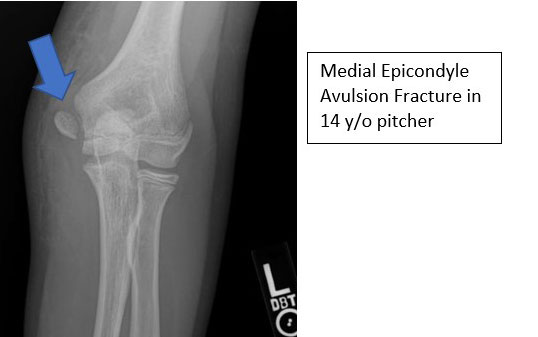
- X-rays demonstrate widening or displacement of the medial epicondyle
- Treatment is based on the amount of displacement and patient’s activities

Treatment
NON-SURGICAL
- For injuries that are non-displaced, and the elbow remains in good alignment then non-operative treatment can be implemented. This treatment includes:
- Bracing/Casting to immobilize the elbow
- Follow-up x-rays to ensure appropriate healing
- Physical Therapy to regain motion
- Return to play throwing program
- Throwing can begin once strength is symmetric and patient is completely symptom free

If left untreated, medial epicondyle fractures can develop into a nonunion
SURGICAL
- For patients that have failed nonoperative treatment or have displaced avulsion fractures, surgery is indicated
- Displacement of the medial epicondyle leads to an unloaded ligament that will atrophy and alter the mechanics of the elbow
- Some studies suggest that even 2mm of displacement can lead to permanent loss of tension of the UCL in the throwing athlete
- Surgical treatment typically involves open reduction and internal fixation with screw placement across the fractured bone
- The patient is typically in an elbow brace for 6 weeks postop with early physical therapy to regain motion
- Patient is released to play once fracture has healed and patient has successfully completed therapy and a throwing program
- In general, medial epicondyle fractures are better treated surgically in the throwing athlete to allow earlier motion, less stiffness and earlier return to sporting activity with decreased chance of nonunion.

Medial Epicondyle ORIF PostOp Protocol
You will need the Adobe Reader to view and print these documents. 